

 Orofacial injuries are very common and are a result of afflictions of many types. Except in traffic accidents, fights, unfortunate incidents, occupational accidents, injuries also happen in sport. All of them, including orofacial ones, happen often, no matter the athlete’s physical shape, his attention as well as the usage of protecting equipment. These injuries happen especially in various contact sports, among which are martial arts.
Orofacial injuries are very common and are a result of afflictions of many types. Except in traffic accidents, fights, unfortunate incidents, occupational accidents, injuries also happen in sport. All of them, including orofacial ones, happen often, no matter the athlete’s physical shape, his attention as well as the usage of protecting equipment. These injuries happen especially in various contact sports, among which are martial arts.
In martial arts and sports training it is very important to reduce (if one cannot totally exclude) the risk of injury. The majority of injuries happen for predictable reasons which can be influenced and prevented. Many factors contribute to the frequency and gravity of the injury, some of which are athlete’s good physical and mental preparation, technical and tactical perfection, his experience as well as the choice of the right protecting equipment.
Preventive measures for the development of orofacial injuries in martial arts include the usage of various types of protecting equipment; extraoral (mostly in fencing), interdental (intraoral) and, in rare cases, a combined mouthguard for the mouth and teeth. Interdental protectors are usually used in martial arts and in sports and can be finished, semi-finished (semi-guard) or made individually. Interdental protectors take on a diverse role in preventing various orofacial injuries in martial arts and sport in general.

Martial arts are viewed as high-risk or extreme sports so the usage of mouthguards during training is recommended. However, for most martial arts, those mouthguards have become obligatory. It needs to be emphasized that mouthguards have to be used in recreational as well as competitive sports, equally consistently during trainings and competitions.
For example, in the United States of America according to the information given by the National Youth Sports Foundation for Safety, 5 million teeth are broken each year. Out of all injuries, tooth injuries happen in 40% of cases. When it comes to tooth injuries in martial arts, it is usually the front teeth that are broken, especially the central upper or lower teeth.
Because of a great number of orofacial injuries, various studies have been made in many countries across the globe and their aim is to prevent and protect sportsmen from these kind of injuries. This article will mention a few significant ones- Denmark (J. Sane, J.J. Raun, 1988), Australia (Sydney, 1990), Sweden and Switzerland (J.P. Schatz, Geneva, 1993), United Kingdom (P.J.Chapman, London, 1993), USA (American Dental Association, M.Bhat, R. Flanders, Illinois, 1995), Japan (T. Yamada,Y. Sawaki, I. Tohnai, Tokyo, 1998) , Switzerland and Germany (A. Filipi, B. Lang, Stuttgart, 2002), Israel (L.Levin, M.Baydar, 2003), Brasil (AC Da Silva, Rio da Janeiro, 2004), Turkey (M. Ozbek, I. Tulunoglu, 2004; G. Shirani, Istanbul, 2010), Austria and Italy (Y. Pohl, Vienna, 2008), France and England (A. Bozio, Paris and S. Brecker, London, 2010), Russia (V. Roginsky, Moskow, 2011), Central India (V. Tiwari, A. Singh, 2014), Croatia (V. Jerolimov, V. Bubalo, Zagreb, 2015).
Protection of the whole face by using, for example, helmets, maska or face protectors (extraoral and combined protectors) is not possible in most martial arts disciplines. This is why an effective prevention of tooth, jaw, joint or soft tissue injuries can be achieved with the help of a well-adjusted interdental (intraoral) protectors (i.e. mouthguards). First such mouthguards started to be used back in 1913. They were originally used only in boxing; the first mouthguard was invented by an English dentist, Woolf Krause, and his son Phillip in 1892. Half a century later it began to be used in other martial arts skills and sports, first in French boxing-savate, then in Muay-Thay and in point karate, i.e. kick-boxing and tae- kwon-do. The usage later spread to other sport disciplines. During the second half of the 20th century, the types and shapes of the mouthguard as well as the technology and materials used in its production have started to be explored and researched more seriously, mostly in the USA.

Mouthguards are special devices made out of a material similar to hard rubber. This material can absorb shock, i.e. the power of the blow and prevents its further spread on dental and bone structures. Three types of interdental mouthguards exist-finished (universal) which are produced in two sizes and are of the worst quality. Then, the semi- finished (semi-guard, “boil and bite“) which need to be put into boiling water and placed into the mouth after they have cooled down in order to adjust to the teeth, i.e. the jaw. Finally, the individual mouthguards are made at the dentist’s office and are of the best quliaty.
Finished mouthguards are the cheapest and can be bought in pharmacies or in shops that sell sports equipment. Factories standardize them in two (universal) sizes which is why they usually don’t adapt well to the teeth and, consequently, often fall out. Talking and breathing with such mouthguards is also hampered and their role to protect is also quite questionable. Athletes usually feel uncomfortable while using such protectors. Today, they are used more rarely, mostly in poorer countries
Semi-guards are more expensive and can also be found in pharmacies and sports equipment shops. An athlete need to prepare such mouthguards to his own teeth and jaw structure. They are shaped like a rubber cylinder which needs to be placed into boiling water and keep it immersed for a maximum of one minute (see the manufacturer’s instructions) so it can soften. Then it needs to be taken out and put under a stream of cooler water. The person using the mouthguard has to centre it in his mouth and bite into it, then hold for a couple of minutes. He needs to make sure that the mouthguard is already cooled in order not to burn himself. When it comes to this type of mouthguards, the place where the teeth make the biggest force, i.e. where the bite is the strongest is the place where the mouthguard’s thickness will be the smallest. Its protection here is questionable. Some manufacturers tend to produce thicker mouthguards which, as a result, make it difficult to breathe, speak and can be uncomfortable to wear. The CustMbite MVP (semi-guard) is a higher-quality mouthguard which was approved by the ADA (American Dental Association).
Individual mouthguards are made in the dentist’s office and, in order to have them customly made, an athlete needs to plan two or three appointments. He and the dentist need to agree on the material and the color, one of the three types of production, its maintenance and, most importantly, take a good imprint of the teeth. The cost range of such mouthguards in Europe goes from 100 to 150 euros (around 200 dollars) and the reason why they are so expensive is that those mouthguards consist of more layers (usually two or three layers). Producing a mouthguard in more layers is very important because only layered materials have the ability to diminish the punch and evenly distribute the power of the blow. Thicker individual moutguards can also be produced and they are made according to the wish of the athlete (depending on the sport, i.e. the harshness of the discipline he trains) and are usually made out of three layers of material. It is very important to adjust the mouthguard to the teeth as well as making sure it does not bother the person wearing it.
It is important to wash the mouthguard each time before and after using it. It needs to be washed meticulously with a brush and toothpaste. It is best to carry it in a box with small holes which will assure its proper ventilation and prevent the development and spread of bacteria. Also, the box needs to be washed with soap and water from time to time. The mouthguard has to be protected from an immediate source of heat and it shouldn’t be placed under direct sunlight. When washing the mouthguard, it shouldn’t be rinsed in hot water because its shape could change and transform. When visiting your dentist, take your mouthguard with you so he can inspect it and check if everything is alright with it.
It is not wise to use damaged or old (worn-out) mouthguards because making a new, even the most expensive one will cost you less than to cure minor orofacial injuries at your dentist’s office. Children and teenagers need to change their mouthguards more regularly because their teeth and jaw develops as they grow. Used with proper care, finished and semi-finished mouthguards have an expiry date that last for a year (or a maximum of a year and a half). However, higher-quality individual mouthguards can last up to two years when maintained properly. If you are using a mouthguard longer than mentioned, it is most likely old and worn-out, i.e. faulty and inoperable.
It is important to stress that interdental protectors don’t guard only the teeth and the surrounding soft tissue, but also stabilize and preserve the temporomandibular joints (TMJ) from injuries. They also reduce the number and gravity of head and neck injuries because they successfully absorb the power of the blows given to the lower jaw which are then conveyed on a smaller rate to the skull bones and their harm is significantly decreased.
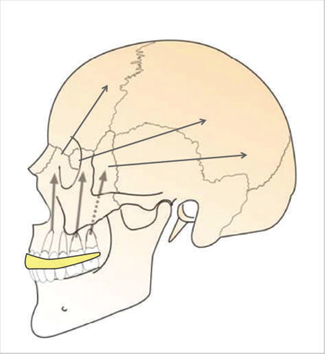
Further on, they protect surrounding soft tissue (cheeks, lips and tongue) from injuries inflicted by the sharp corners of the teeth, especially the upper jaw. Using mouthguards can also reduce the likelihood of rupture or movement of the central teeth because of direct punches as well as the back teeth which suffer during abrupt crashes between dental arches of the upper and lower jaws. Using a mouthguard also reduces the chance of fracture of the upper jaw as well as injuries of the lower jaw. It lessens the force of the hit by absorbing it and transmitting it at a reduced amount to the surrounding bone structures. Mouthguards also prevent the movement in the lower jaw joint, i.e. TMJ backwards (towards the base of the skull), therefore reduce the risk of deformation of the joint itself as well as the bounding bone structures. By weakening the force of the hit, interdental protectors reduce the chance of brain concussion and cervical spine injuries. Namely, when receiving a hit on the lower jaw, thanks to the firm grasp between the dental arches and the interdental protector, an additional activation and contraction of the head and neck muscles occurs. Thereby, during such hits, a resistance to the rotational forces increases and the possibility to get a concussion is twice smaller. Also, mouthguards contribute to an athlete’s increase in self-confidence, a better focus and a higher-quality of sports performance.
In martial arts, injuries of the TMJ can occur by hitting the joint directly or indirectly hitting the chin or the side of the lower jaw where the force is transferred on to one or both joints. Sometimes, in certain martial arts, injuries and deformities of the TMJ can be a result or frequent and often unnoticeable exertion as well as the load of the TMJ and the surrounding tissue.
A person whose tooth has been broken can be in a “knock down“ state and he should be reanimated, i.e. given CPR. If the person’s mouth is clogged with blood and a broken tooth he will need to be given mouth-to-nose rescue breathing.
In case of a broken or knocked out tooth carefully wash the surrounding area of the injured spot, stop the bleeding with a gauze or a clean piece of clothing and put a cold compress against that place. If it is dirty, wash the knocked out tooth under a light stream of water, but by all means do not scrape the dirt with a brush. It is best to place the tooth in a contact lens solution. In case you do not have the solution at your disposal, put the tooth in a container with milk, water or place it under the tongue (it is important for it not to dry out) and urgently go to your nearest dentist (it is best if it is done in under 30 minutes).
Damages of the teeth and the surrounding supporting structures are sudden. The patients who come to hospital with those kind of injuries are mostly emergency cases where the time is limited. The period between the event of the injury and the medical procedure is of a crucial importance for the destiny of the tooth and the quality of the healing outcome.
During the first phase of the examination, the doctor will need to have in mind the possibility of the obstruction of the airway with broken teeth, blood, dentures and interdental protectors. After checking the airways, the function of the vascular system also needs to be inspected. Furthermore, it is necessary to briefly examine the neurological status of the patient by looking into the nerve sensitivity in the TMJ area, time and place orientation as well as the presence of a headache, sleepiness, nausea, an urge to vomit, unconsciousness and amnesia.
Along with the rest, orofacial injuries are the reason of irregular training or even a break in practicing sports and competing. It also needs to be said that a loss of a tooth leads to a permanent functional, esthetic and psychosocial disadvantage in an athlete’s life adding up to high expenses for treatments and, later on, prosthetics.

Sometimes an athlete receives a strong punch in the teeth and, after some time, the swelling recedes and the pain stops. If there hasn’t been a movement inside the jaw or no loose teeth can be found, the person thinks everything is fine. Unfortunately, an injury or a rupture of the root could also have happened so, after some time, the tooth starts to darken in color. The reason why this happens is because microscopical parts of the blood cells which used to feed the tooth remain inside of it. These cells start to disintegrate and release a pigment which gives the tooth a darker color (first it is purple, then grayish and then the tooth turns black). This kind of injury also needs to be resolved and treated in a dentist’s office.
According to the instruction of the Academy for Sports Dentistry in 2010, mouthguards are an obligatory protecting equipment in martial arts in the USA. Today, American Dental Association recommends using mouthguards in martial arts such as wrestling, judo, ju-jutsu, aikido, fencing and archery.
In some martial arts such as fencing, kata performance or in archery, injuries do not occur because of hits or punches, but because of overstraining the masseter muscle and the jaw joints which often leads to their micro traumatic damages, consequently affecting the functional disorders in the orofacial region. However, the main problem with these kinds of injuries is that they are not immediately recognized.
Recently, an international network has begun monitoring risk factors of sports injuries and an internet database has been developed — International Sports Injury System — ISIS. The aim is to improve sports results and reduce the number as well as the gravity of injuries. The ISIS protocol can be used in the majority of martial arts with an objective to follow and compare types of sports injuries. Entering the information in the system is reliable and is based on the usage of the international Classification of Disease (ICD), i.e. using the so-called ICD-10 diagnostic system given by the World Health Organization.






{kind=link}